Mechanisms of Dissociation
clips from cognitive atomization


I was reviewing ideas from Cognitive Atomization and thought that sharing these bits could be useful to people. The introduction to the original formal essay, Desummation, is a bit difficult to read. This extraction of Desummation makes things easier by skipping right to the juicy bits. There are lots of interesting perceptual demonstrations of the concept below, so I hope you enjoy it!
Psychonaut Wiki notes an effect of pattern recognition suppression that is commonly reported on NMDAr antagonists (dissociative drugs). This might explain the lack of the three flash illusion in schizophrenic subjects as this may be a suppression of associating audio and video stimuli together. In a sense, this is a kind of ‘atomization’ effect as well. These two stimuli may normally summate due to close temporal proximity of occurrence. If coincidence detection relies on NMDAr, then blocking NMDAr may prevent awareness of coincident occurrences, such as in the three flash illusion. The Wiki notes that this is very similar to the apperceptive agnosia (PsychonautWiki).

Apperceptive agnosia is the failure to recognize visual objects and a failure of visual coherence. In some sense, all recognized objects could be viewed as illusions of a sort. External reality may not be so ‘representational’ in reality, but representations help us navigate the world. In the same way that illusions fail to occur in schizophrenic subjects, you could imagine that all representational models fall apart at the farthest end of this spectrum of phenomena. In the totally atomized state, visual information may become without recognized patterns, instead with an immense perception of distinct pixels. The spectrum of visual changes that occurs between illusions/hyper-recognition of patterns to totally atomized pixels of perceptual qualia might reveal the structure and organization of perceptual patterns themselves. It may reveal which patterns are more significant than others or the order in which layers of illusions are organized into the kinds of representations that we are used to observing. The NMDAr antagonists may dose-dependently strip away these illusions until we reach a state of total agnosia. Cognitive atomization could be defined as agnosification of the mind in some sense. You could imagine that this occurs not only in perception but with cognition generally.
There is an important consideration and nuance that should be clarified here about illusions and visual distortions. We should distinguish agnosiac perceptions from illusions in future research because at the moment it appears that visual changes may generally be labeled as ‘illusions’ in some of the research that describes the effects of ketamine or similar drugs. One might view the agnosiac state to be full of ‘illusions’ but the very opposite may be true. Cautiously classifying and distinguishing visual alterations will be important in the future of research on perception.
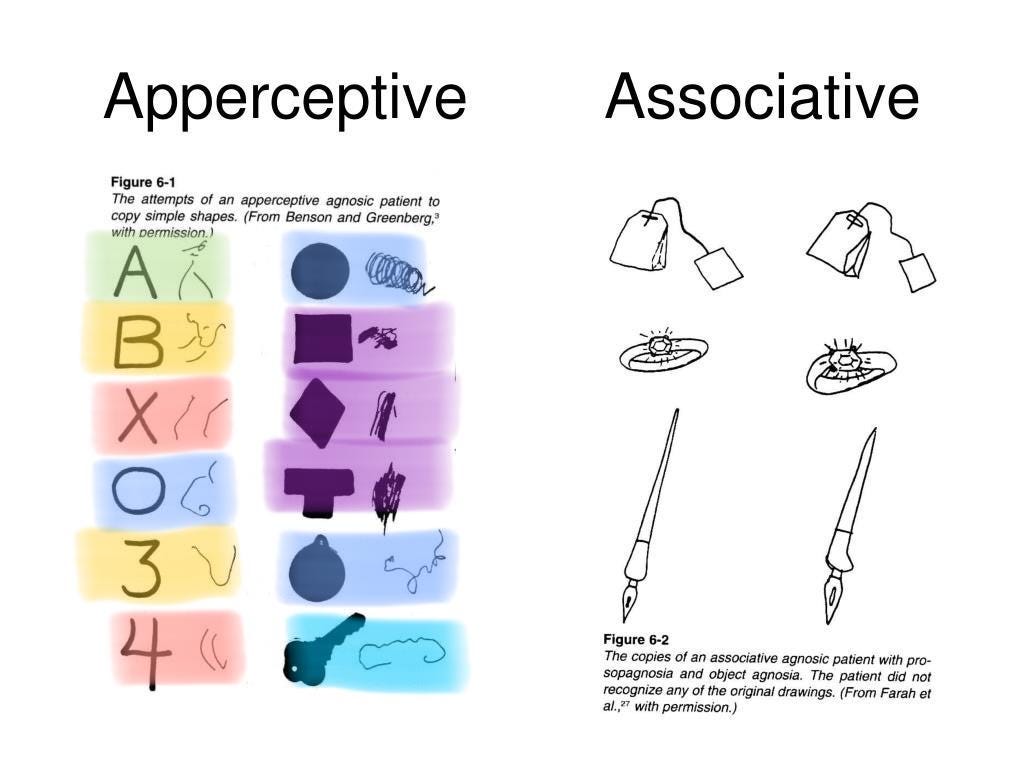
This is an interesting chart that is accessible on Google images. I’ve color-labeled objects that appear to have consistencies both in the normal view and the agnosic representation drawing. Notice the X and 4 share the property of being 2 lines. Indeed a normal 4 involves an X shape. The circle representations tend to be strange spirals here. The agnosic A appears to be two lines, much like the 4 and the X, but with a circle representation at the top. 3 and B both normally share the same double curve shape, and the agnosic representations here also share a strange curve-like shape. Perhaps this indicates a failure of spatial summation and the loss of illusions in psychosis could be likened to a very mild form of agnosia. NMDAr antagonists may dose-dependently induce agnosia-like effects.
If you are enjoying this so far, please share it with friends who might be interested :)
Illusions
Illusions may be able to be viewed as something opposite of cognitive atomization. Cognitive hyper-integration, predictive perception, and an automated representation of the external world.
There are a few illusions that schizophrenics have been shown to sometimes have immunity to. This might suggest an involvement of NMDAr in the development of illusions, perhaps as a form of perceptual learning and associative prediction. There are five illusions I found in the research that schizophrenics have immunity to in the literature. This includes the inverted mask illusion (Dima, Roiser, Dietrich et al 2009), the Chubb illusion (Dakin, Carlin, & Hemsley 2005), the Muller-Lyer illusion (Shoshina, Perevozchikova, Konkina et al 2011), the Ebbinghaus illusion (Silverstein, Keane, Feigenson et al 2013), and lastly the ‘three flash’ illusion (Norton, Ongur, Stromeyer III, & Chen 2008). These illusions may be learned/conditioned visual perception ‘habits’ that have formed in response to repeating and consistent patterns of observations, such as basic dimensionality, laws of shapes, distance, motion, and so on. Since reality never presents us with a contradicting perception, our brain learns to automatically assume certain kinds of visual information to exist in the world that doesn’t match with what kind of signals are actually entering the visual system from the external world. For example, the inverted mask illusion reveals that we will perceive a face with inverted 3D data as a regular forward-facing face. This is because we never see inverted faces and thus we can assume that the face is facing towards us, as it always is.

This may cause us to disregard external information and assume information to be present as a cognitive tool of efficiency. This may reduce the load that processing vision takes on our conscious processing by automating our response to a small set of cues from the external environment by using a kind of perceptual memory recall rather than analyzing the present environment as if it were unfamiliar. It is a form of stereotyping that helps us simplify processing and ignore much of the external data, relying mostly on memories of how the external data is and only regarding very little external information, such as minimal shading or bifocal spatial data.
Presumably, an illusion like the motion aftereffect relies on more short-term kinds of memory and predictions, in which a repeating motion pattern becomes predictable and assumed to continue even when the source of motion ceases. The perceived continuation of motion seems to make the walls or surrounding objects change shape, move and drift. The initial motion source may condition visual processing and induce a learned motion effect that is very short-term and fleeting. On the other hand, an illusion like the inverted face mask may not rely on such short-term memories, but instead, involve long-term memory for face-like 3D structures and their repeating shapes conditioning one’s expectations for 3D shape in the assessment of present-moment face-like stimuli. Those with schizophrenia might have impaired long-term learning due to chronically impaired short-term memory mediated by hypofunction of NMDAr. Using NMDAr antagonists to test people’s responses to different kinds of illusions might reveal distinctions between long-term recall versus immediate learning being blocked. If NMDAr antagonism induces immunity to long-term kinds of illusions, this may reveal at least some alteration to recall of long-term visual memory.
Another illusion, known as the three-flash illusion, also tends to not trick those with schizophrenia. This illusion involves a video of 2 visual blips paired with 3 auditory blips. For most people, this video appears to present 3 three visual blips, possibly due to the audio associating to the visual effect. This can be related to summation in which the sound and the audio might be assumed to be associated, as if the blinking causes the sound. Because we hear the 3 sounds clearly, we assume our visual system missed one of the blinks, as these are far harder to notice and occur in such short time periods. In schizophrenia, this may be impaired much like associative learning is impaired. The visual and auditory events may appear to occur as distinct events, non-associated, and essentially atomized into separate experiential pieces. This seems to relate to the concepts of summation and prepulse inhibition, which both involve temporally close events being associated and reacted to and may rely on NMDAr activation. If a loss of NMDAr activity results in such an atomized experience, it could hypothetically impair cue-responses that depend on summated cues. So for example, the recognition of an object may require that lower layers of perception form associations, such as the surfaces that associate to create that 3D object. If one does not recognize lower layers as associated, maybe there is an absence of the cue for recognizing a familiar object. This may open the door to misperceptions. It is worth noting that perhaps objects will often still be recognized but require more processing and involve less perceptual shortcuts, taking up more space for working memory, ultimately reducing awareness capacity through information overload.
It is important to note that cannabis has also been linked to illusion immunity (Koethe, Gerth, Neatby et al 2006). Cannabis has also been shown to induce psychotic symptoms very frequently, even in non-schizophrenic subjects (D’Souza, Sewell, & Ranganathan, 2009). The psychoactive effects could be seen as often being a desirable set of psychotic effects, we should be cautious in defining ‘psychotic symptoms’ as inherently bad reactions to the drug, but rather descriptive reactions to the drug. Another study found that an NMDAr antagonist, MK-801, produces a reduction in sensitivity to the Muller-Lyer illusion in capchaun monkeys (Jacobsen, Barros, & Maior, 2017). The sensitivity to this illusion is thought to differ by culture, urban versus rural (Ahluwalia 1978). This suggests that the illusion is learned and is likely a kind of visual long-term memory. This supports the hypothesis that the effects of NMDAr antagonists involve disruption recall of long-term memory, at least perceptually. The application of the drug seems to reverse visual conditioning or visual learning that produces these illusions.

The inverted mask illusion (as well as the other illusions) may involve a conditioned response in which a visual cue made up of associations elicit a learned habitual representation in perception. For the inverted mask illusion, this involves a habitual representation that is generated in response to common cues of the physical structures of a face, including lighting and shadows. This can be likened to a perceptual auto-correct system. In text-based autocorrect on mobile devices, we observe the wrong word being recalled based on the expectation and prediction of that word belonging within the sentence’s context. These context words bias the expectation of what word is correct by associating the context to a list of words that you might be typing and choosing the most likely word that matches with the most frequent expected word. We observe these auto-correct systems failing us, which is similar to the way our brain pulls up the wrong perception or as we call it, an illusion. The loss of illusions from NMDAr antagonists and schizophrenia might suggest a loss of predictive perception processes, an absence of memory access to retrieve these predicted perceptions.
If you liked this, you can read the full argument here. The citations are all included in that link as well.
I’d also be curious to hear if this theory resonates with your experience of dissociative drugs.